
Plagiocephaly Flat Head Syndrome Symptoms, Causes, Types & Treatment
Plagiocephaly flat head syndrome symptoms causes types and treatment – it’s a mouthful, isn’t it? But understanding this condition is crucial for parents and caregivers of infants. This post dives into the world of plagiocephaly, exploring its various forms, underlying causes, and available treatment options. We’ll unravel the mysteries behind this common head shape abnormality, providing you with clear explanations and practical information to navigate this often-concerning issue.
Get ready to learn everything you need to know about helping your little one develop a healthy head shape!
From the subtle asymmetry of positional plagiocephaly to the more severe cases requiring surgical intervention, we’ll cover the spectrum of this condition. We’ll examine the different diagnostic tools used to identify the type of plagiocephaly, and we’ll delve into the various treatment strategies available, from simple positional changes to more complex medical interventions. This isn’t just about the medical aspects; we’ll also touch on the emotional impact on families and discuss ways to support both the child and their loved ones during this journey.
Plagiocephaly

Source: healthymamahacks.net
Plagiocephaly, often referred to as flat head syndrome, is a condition characterized by an abnormally shaped head, typically asymmetrical. It’s a more common concern than many parents realize, impacting a significant number of infants. Understanding its causes, types, and treatment options is crucial for ensuring the best possible outcome for affected babies.Plagiocephaly’s prevalence varies depending on factors such as healthcare access and reporting practices.
However, studies suggest it affects a considerable percentage of infants, leading to concerns among parents and prompting significant research into prevention and treatment methods. The impact on families can be substantial, involving potential emotional stress related to the child’s appearance, the need for interventions, and the time commitment required for treatment. For some families, there is also the added worry of potential long-term effects, although most cases resolve with appropriate management.
Plagiocephaly Classifications
Plagiocephaly is broadly categorized into three main types, each stemming from different underlying causes. Accurate classification is crucial for determining the appropriate course of treatment.
- Positional Plagiocephaly: This is the most common type, resulting from prolonged pressure on the back or side of the head. This pressure typically occurs when infants spend extended periods lying on their backs, often due to factors like premature birth, torticollis (neck muscle tightness), or sleeping preferences. The skull bones are still malleable at this age, leading to flattening.
The underlying skull shape remains normal.
- Deformational Plagiocephaly: Similar to positional plagiocephaly, deformational plagiocephaly involves an abnormally shaped head due to external pressure. However, it’s characterized by more severe flattening and potential distortion of the underlying skull shape. This often requires more intensive management than positional plagiocephaly.
- Synostotic Plagiocephaly: This is the least common type but potentially the most serious. It results from premature fusion of one or more of the skull’s sutures (the joints between the bones). This premature fusion restricts the skull’s normal growth, leading to significant asymmetry and potential complications. This type usually requires surgical intervention.
Symptoms of Plagiocephaly
Plagiocephaly, or flat head syndrome, presents with noticeable head shape asymmetry. The severity of the flattening varies, impacting the overall appearance and potentially causing other developmental concerns. Recognizing these symptoms is crucial for early intervention and treatment.
Observing the physical characteristics of plagiocephaly requires a careful examination of the head’s shape, ear position, and forehead contour. A noticeable asymmetry is the primary indicator. The affected side of the head will appear flatter than the other, and this flattening can range from mild to severe depending on the extent of the deformation.
Head Asymmetry, Ear Position, and Forehead Shape in Plagiocephaly
The degree of plagiocephaly is often categorized into mild, moderate, and severe based on the observable physical characteristics. The following table summarizes these distinctions:
| Characteristic | Mild Plagiocephaly | Moderate Plagiocephaly | Severe Plagiocephaly |
|---|---|---|---|
| Head Asymmetry | Slight flattening on one side of the head, barely noticeable to the untrained eye. | Obvious flattening on one side of the head, asymmetry easily visible. | Significant flattening on one side of the head, with a pronounced asymmetry. The head may appear significantly distorted. |
| Ear Position | Slight forward displacement of the ear on the flattened side. | Noticeable forward displacement of the ear on the flattened side. | Significant forward displacement of the ear on the flattened side, potentially with other positional abnormalities. |
| Forehead Shape | Minimal asymmetry in forehead shape. | Slight asymmetry or prominence of the forehead on the opposite side of the flattening. | Significant asymmetry of the forehead, with a noticeable protrusion on the non-flattened side. |
Documenting Plagiocephaly Symptoms for Medical Professionals
Accurate documentation of plagiocephaly symptoms is essential for effective communication with healthcare providers. Parents or caregivers should provide detailed descriptions of the observed characteristics, ideally supported by photographic evidence.
Examples of documentation include:
“My child presents with noticeable flattening of the right side of the head. The right ear appears to be slightly forward compared to the left. The forehead appears slightly more prominent on the left side.”
“Significant asymmetry is observed in my child’s head shape. The left side is significantly flatter than the right. The left ear is noticeably displaced forward, and the right side of the forehead protrudes significantly.”
Including precise measurements, if available, enhances the accuracy of the documentation. For instance, specifying the degree of asymmetry using photographs taken from various angles and noting the measurements of the head circumference at different points would provide a more complete picture for the medical professional.
Causes of Plagiocephaly
Plagiocephaly, the flattening of the head, arises from a variety of factors, broadly categorized into positional, deformational, and synostotic forms. Understanding these causes is crucial for appropriate diagnosis and management. The severity and type of plagiocephaly significantly influence the treatment approach.
Positional Plagiocephaly
Positional plagiocephaly is the most common type, resulting primarily from external forces applied to the developing skull. Prolonged pressure on one side of the head, often due to sleeping position, can lead to flattening. This is particularly prevalent in infants who spend extended periods lying on their backs, especially if they have limited neck muscle control or a preference for turning their head to one side.
Uterine constraint, where the baby’s head is compressed within the womb, can also contribute to positional plagiocephaly, although this is less frequent. The pressure on the skull causes the bone to remodel, leading to the characteristic asymmetry. Early intervention, such as encouraging tummy time and changes in sleeping position, is often sufficient to correct this type.
Deformational Plagiocephaly
Deformational plagiocephaly encompasses a broader range of factors contributing to head shape abnormalities. While positional factors play a significant role, genetic predisposition and other environmental influences also come into play. For example, certain genetic variations might influence the skull’s resilience or the development of neck muscles, increasing susceptibility to flattening. Furthermore, prematurity, low birth weight, and conditions affecting muscle tone (like hypotonia) can make infants more vulnerable to developing deformational plagiocephaly.
These factors can interact and amplify the effects of prolonged pressure on the skull.
Synostotic Plagiocephaly (Craniosynostosis)
Synostotic plagiocephaly, in contrast to positional and deformational forms, is caused by the premature fusion of one or more of the cranial sutures – the fibrous joints connecting the bones of the skull. This premature fusion restricts the skull’s normal growth, leading to asymmetrical head shape. The specific suture involved dictates the pattern of the skull deformation. For instance, premature closure of the lambdoid suture (at the back of the head) often results in a flattened occipital bone on one side and posterior displacement of the ear on the same side.
This condition is often diagnosed at birth or in early infancy and may require surgical intervention to correct the fused suture and allow for normal skull growth. The underlying cause of craniosynostosis is often genetic, though sometimes it can be associated with specific syndromes or other medical conditions.
Types of Plagiocephaly
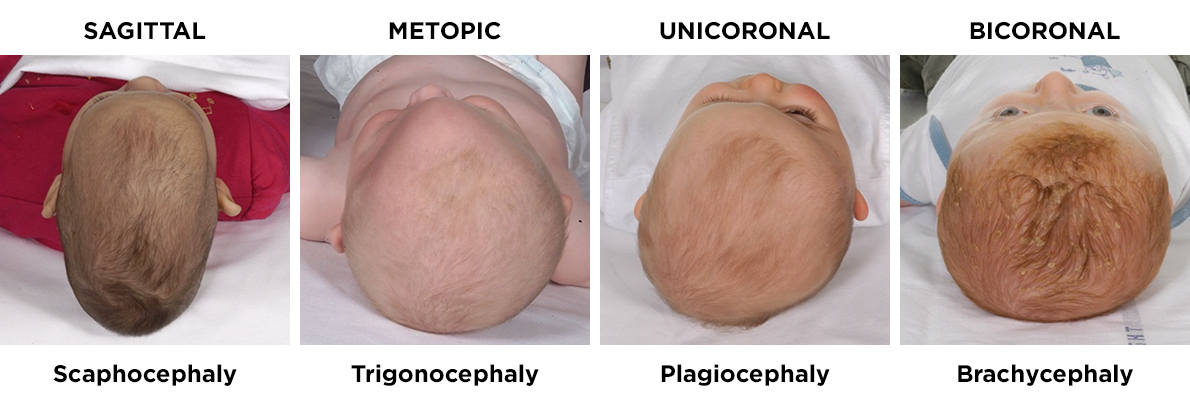
Source: co.uk
Understanding the different types of plagiocephaly is crucial for appropriate diagnosis and treatment. While all types result in a misshapen head, the underlying causes and therefore the best approaches to management vary significantly. Misdiagnosis can lead to delayed or inappropriate interventions, highlighting the importance of accurate classification.
Plagiocephaly is categorized primarily into three main types: positional, deformational, and synostotic. These types differ significantly in their etiology, severity, and the long-term outlook for the child. While some overlap can exist, careful clinical examination and often imaging studies are necessary to distinguish between them.
Positional Plagiocephaly
Positional plagiocephaly is the most common type, resulting from prolonged pressure on the back or side of the head. This is often caused by factors like sleeping position, particularly in infants who spend extended periods lying on their backs. The skull bones themselves are normal, and the flattening is a consequence of external forces. The prognosis is generally excellent with conservative management, such as repositioning and tummy time.
Understanding plagiocephaly, from its telltale flattened head shape to the various treatment options available, requires a holistic approach. Proper nutrition plays a vital role in a baby’s development, and I found this article on are women and men receptive of different types of food and game changing superfoods for women incredibly insightful, as it highlights the importance of tailored diets.
This understanding extends to managing plagiocephaly, ensuring optimal development and minimizing long-term effects.
Severity is usually mild to moderate, characterized by asymmetry but without significant bone deformation.
Deformational Plagiocephaly
Deformational plagiocephaly shares some similarities with positional plagiocephaly in that it involves skull asymmetry without underlying bone fusion. However, it tends to be more severe and involves a wider range of skull deformities. The etiology is often multifactorial, potentially involving factors like intrauterine constraint, premature birth, or underlying muscle imbalances. Unlike positional plagiocephaly, simple repositioning is often insufficient to correct deformational plagiocephaly.
Treatment may involve helmet therapy to reshape the skull. The prognosis is generally good with appropriate intervention, but the severity and the need for intervention can be greater than with positional plagiocephaly.
Synostotic Plagiocephaly
Synostotic plagiocephaly, also known as craniosynostosis, is a much more serious condition. It results from the premature fusion of one or more cranial sutures, the fibrous joints connecting the skull bones. This premature fusion restricts the normal growth of the skull, leading to characteristic head shape deformities that are often more severe and complex than those seen in positional or deformational plagiocephaly.
Unlike the other types, it is not simply a flattening but rather a change in the underlying skull bone structure. This condition requires surgical intervention to correct the fused sutures and allow for normal skull growth. The prognosis is generally good with early surgical correction, but untreated synostotic plagiocephaly can lead to significant cosmetic and neurological complications.
Distinguishing Features of Plagiocephaly Types
The following list summarizes the key distinguishing features of each type of plagiocephaly to aid in understanding their differences.
- Positional Plagiocephaly: Mild to moderate asymmetry, caused by external pressure, responds well to conservative management, excellent prognosis.
- Deformational Plagiocephaly: More severe asymmetry than positional, multifactorial etiology, may require helmet therapy, good prognosis with intervention.
- Synostotic Plagiocephaly: Premature fusion of cranial sutures, significant skull deformation, requires surgical intervention, good prognosis with early surgery.
Diagnostic Pathway for Plagiocephaly
A flowchart can help visualize the diagnostic process to differentiate between the types of plagiocephaly. This is a simplified representation, and a thorough clinical evaluation is always necessary.
Imagine a flowchart. It would begin with “Infant presents with suspected plagiocephaly.” The first branching point would be “Is there evidence of premature cranial suture fusion?” A “yes” answer would lead to “Synostotic Plagiocephaly,” requiring imaging studies and surgical consultation. A “no” answer would lead to the next branching point: “Is the asymmetry mild and responsive to repositioning?” A “yes” answer leads to “Positional Plagiocephaly,” with conservative management recommended.
A “no” answer suggests “Deformational Plagiocephaly,” potentially necessitating further evaluation and possibly helmet therapy.
Diagnosis and Assessment of Plagiocephaly
Diagnosing plagiocephaly involves a careful assessment of the baby’s head shape and a thorough evaluation to rule out other underlying conditions. This process typically combines a physical examination with imaging techniques, providing a comprehensive understanding of the head’s asymmetry and any potential complications.
Physical Examination
A physical examination forms the cornerstone of plagiocephaly diagnosis. The healthcare provider will carefully examine the baby’s head, noting the shape, size, and any noticeable asymmetry. They will palpate the skull to feel for any bony abnormalities or suture closures. The examiner will look for flattening on one side of the head, and potential ear displacement or asymmetry of the facial features.
The overall head circumference will be measured and compared to growth charts to determine if it falls within the normal range. This visual and tactile assessment is crucial in determining the severity and type of plagiocephaly.
Cranial Ultrasound
Cranial ultrasound is a non-invasive imaging technique often used to assess the skull’s bones and brain structures in infants. It utilizes high-frequency sound waves to create images of the soft tissues and bones of the head. This technique is particularly useful in identifying any underlying issues that might contribute to plagiocephaly, such as craniosynostosis (premature fusion of the skull bones).
Cranial ultrasound allows for visualization of the sutures and brain tissue, helping to differentiate between positional plagiocephaly (deformational) and craniosynostosis (synostotic). It is a safe and effective method for evaluating infants, especially those who are too young for other imaging techniques.
Role of CT and MRI Scans
While cranial ultrasound is typically sufficient for diagnosing most cases of plagiocephaly, CT (computed tomography) and MRI (magnetic resonance imaging) scans may be necessary in certain situations. These techniques provide more detailed images of the skull and brain. CT scans are particularly useful in visualizing bone structures, while MRI scans provide excellent images of soft tissues. These scans are often used to confirm the diagnosis of craniosynostosis, where premature fusion of the skull bones is suspected.
They help identify the specific sutures involved and assess the extent of the fusion. These are generally reserved for cases where cranial ultrasound findings are inconclusive or suggest a more complex underlying condition. For example, if a cranial ultrasound shows a suspicious suture, a CT scan could be used to confirm the presence and extent of craniosynostosis.
Understanding plagiocephaly, from its telltale flattened head shape to the various treatment options available, is crucial for parents. While researching this, I stumbled upon a fascinating article exploring how early detection of conditions like dementia might be possible, like checking for signs in the eyes as discussed in this article: can eye test detect dementia risk in older adults.
It made me think about how early intervention is key for both plagiocephaly and other potential health issues later in life. Early diagnosis and treatment for plagiocephaly can significantly improve outcomes.
Cephalic Index and its Significance
The cephalic index is a crucial measurement used to quantify head shape asymmetry. It’s calculated using the following formula:
Cephalic Index = (Maximum head breadth / Maximum head length) x 100
The cephalic index provides a numerical value representing the head’s shape. A cephalic index below 75 indicates a dolichocephalic (long and narrow) head, while a value above 85 suggests a brachycephalic (short and wide) head. Deviations from the normal range, along with visual assessment of the head’s asymmetry, help determine the severity of plagiocephaly. For example, a child with a significantly asymmetric head shape might have a cephalic index that falls outside the normal range, confirming the diagnosis of plagiocephaly and guiding treatment decisions.
The index, however, is only one aspect of the assessment and should be considered alongside other clinical findings.
Treatment Options for Plagiocephaly: Plagiocephaly Flat Head Syndrome Symptoms Causes Types And Treatment
Plagiocephaly treatment depends heavily on the underlying cause and the severity of the head shape deformity. While some cases resolve spontaneously, others require intervention to prevent long-term cosmetic or functional issues. The approach is generally conservative initially, progressing to more intensive methods if needed.
Conservative Management of Positional Plagiocephaly
Positional plagiocephaly, the most common type, often responds well to conservative management. This focuses on altering the baby’s sleeping position and increasing tummy time. The goal is to encourage the baby to turn their head away from the flattened side and use their neck muscles more, thus redistributing pressure on the skull. This might involve strategically placing toys and objects out of reach to encourage head turning.
Parents are usually advised to place their baby to sleep on their back, but to actively change the baby’s head position during awake periods. Frequent changes in the baby’s position throughout the day are crucial for success. Regular monitoring by a pediatrician is essential to track progress.
Cranial Orthoses (Helmets) for Deformational Plagiocephaly
For moderate to severe deformational plagiocephaly, a cranial orthosis, commonly known as a helmet, is often recommended. These custom-made helmets gently reshape the skull by applying pressure to the prominent areas while allowing normal growth in other areas. The helmet is typically worn for 23 hours a day for several months, with the duration varying depending on the severity of the deformity and the child’s age.
The helmet’s design is personalized to address the specific asymmetry of the skull. While effective, helmet therapy requires commitment from both parents and the child, and regular adjustments may be necessary as the baby grows. A significant improvement in head shape is usually observed, but long-term effects can vary. For example, a study published in the journal
Pediatric Neurosurgery* showed that helmet therapy was effective in improving head shape asymmetry in 85% of infants.
Surgical Interventions for Synostotic Plagiocephaly
Synostotic plagiocephaly, resulting from premature fusion of the skull bones, typically requires surgical intervention. Craniofacial surgery is performed to correct the fused sutures, allowing for normal skull growth. The specific surgical procedure depends on the location and extent of the suture fusion. The surgery involves opening the skull, separating the fused bones, and reshaping the skull to improve its symmetry.
Post-operative care includes monitoring for infection, managing pain, and potentially using a helmet to further refine the head shape. Surgical intervention aims to restore normal skull growth and improve the cosmetic outcome. The success rate of craniofacial surgery for synostotic plagiocephaly is generally high, with excellent results in most cases. However, potential risks associated with any surgery must be carefully considered.
Long-Term Outcomes and Prognosis
The long-term effects of plagiocephaly depend largely on the severity of the deformity and the timeliness and effectiveness of treatment. While many cases resolve well with intervention, understanding the potential long-term implications is crucial for parents and caregivers. Untreated or inadequately treated plagiocephaly can lead to a range of issues extending beyond infancy.Early intervention, typically within the first few months of life, is key to maximizing positive outcomes.
The success of treatment, whether it involves repositioning, cranial molding helmets, or other therapies, varies depending on factors such as the age of the child at the start of treatment, the severity of the deformity, and the adherence to the prescribed treatment plan. The goal isn’t just to correct the head shape but also to mitigate potential long-term consequences.
Cosmetic Concerns
While many children experience significant improvement in head shape following treatment, some residual asymmetry may remain. This can be a source of cosmetic concern for some individuals as they grow older, potentially affecting their self-esteem and confidence. The degree of residual asymmetry varies widely, depending on factors such as the severity of the initial deformity, the age at which treatment began, and the individual’s response to therapy.
In some cases, minor cosmetic imperfections may be barely noticeable, while in others, more noticeable asymmetry might persist. For example, a child with severe plagiocephaly treated later in infancy might still exhibit a slightly flatter area on one side of the head even after successful helmet therapy.
Psychosocial Impact
The psychosocial impact of plagiocephaly can be significant, particularly if the child experiences teasing or bullying due to their head shape. This is especially true if the deformity is noticeable and hasn’t been adequately addressed. Children with untreated or poorly treated plagiocephaly may experience low self-esteem, anxiety, or social withdrawal. The emotional well-being of the child should be considered alongside the physical aspects of treatment.
Early identification and intervention, combined with supportive parenting and potentially professional counseling, can help mitigate these potential psychosocial effects. A child who receives early and effective treatment is less likely to experience such negative impacts.
Success Rates of Treatment Methods
The success rate of plagiocephaly treatment varies depending on the method used and the severity of the condition. Cranial molding helmets, for instance, have shown high success rates in correcting moderate to severe deformities when implemented early. Studies have indicated that a significant majority of infants treated with helmets show marked improvement in head shape. However, complete correction is not always guaranteed, and some residual asymmetry might remain.
Similarly, repositioning techniques, when used diligently and consistently, can be effective in milder cases. However, the success of repositioning is heavily dependent on parental compliance and the timing of intervention. The effectiveness of any treatment is enhanced by early intervention, consistent adherence to the treatment plan, and regular monitoring by healthcare professionals.
Prevention of Plagiocephaly

Source: blogspot.com
Understanding plagiocephaly, from its telltale flattened head shape to the various treatment options available, is crucial for parents. While researching this, I also stumbled upon some helpful information on managing different neurological conditions in children; for instance, check out this article on strategies to manage Tourette syndrome in children , which highlights the importance of early intervention and tailored approaches.
Returning to plagiocephaly, early diagnosis and intervention, such as cranial remolding therapy, are key to achieving the best outcomes.
Preventing plagiocephaly, particularly positional plagiocephaly, focuses on minimizing the pressure on the back or side of an infant’s head. Early intervention and proactive strategies are key to promoting healthy head shape development. By understanding the risk factors and implementing simple preventative measures, parents can significantly reduce the chances of their baby developing this condition.Parents can take several steps to minimize the risk of positional plagiocephaly.
The most effective strategies involve encouraging varied head positions and promoting tummy time, all while ensuring safe sleeping practices. This approach not only helps prevent flat head syndrome but also contributes to the overall healthy development of the infant.
Safe Sleeping Practices to Reduce Plagiocephaly Risk, Plagiocephaly flat head syndrome symptoms causes types and treatment
Safe sleep practices are paramount in preventing plagiocephaly. Always placing your baby on their back to sleep is crucial for reducing the risk of Sudden Infant Death Syndrome (SIDS). However, simply placing your baby on their back isn’t enough; consistent changes in head position are also vital.
- Place your baby on their back for sleep on a firm, flat surface.
- Avoid using soft bedding, pillows, bumpers, or loose blankets in the crib.
- Rotate your baby’s head position during sleep. For example, if they tend to favor sleeping with their head turned to the right, gently reposition them to sleep with their head turned to the left during subsequent naps or nighttime sleep periods.
- Ensure the crib mattress is firm and fits snugly to avoid any gaps where your baby could become trapped.
Promoting Tummy Time for Healthy Head Shape Development
Tummy time is essential for strengthening neck and shoulder muscles, which in turn helps to prevent the development of plagiocephaly. It also stimulates development in other areas. Supervise your baby closely during tummy time, and always place them on a safe, clean surface.
- Start tummy time sessions short and gradually increase the duration as your baby gets stronger. Begin with a few minutes at a time, several times a day.
- Engage your baby during tummy time with toys or interactive activities to keep them entertained and encourage them to lift their head and turn it.
- Offer varied positioning during tummy time, such as on your lap, across your legs, or on a playmat. This encourages different head positions and helps to prevent flattening.
- Don’t force tummy time if your baby is distressed. Instead, try shorter sessions or different positions.
Encouraging Varied Head Positions
Beyond sleep, actively promoting varied head positions throughout the day is crucial. When your baby is awake, try to position them in a way that encourages them to turn their head in different directions. This helps to distribute the pressure on their skull evenly.
- When your baby is awake and in a carrier or car seat, alternate the direction they face.
- During playtime, encourage your baby to look around and reach for toys placed on either side.
- When feeding your baby, alternate the side you hold them on.
- Avoid letting your baby spend excessive time in any one position, especially lying on their back. Encourage them to be on their tummy or in other positions.
Closure
Navigating the world of plagiocephaly can feel overwhelming, but remember you’re not alone. Understanding the different types, causes, and treatment options empowers you to advocate for your child’s well-being. Early detection and appropriate intervention are key to achieving the best possible outcomes. While some cases resolve with simple adjustments, others may require more intensive medical care. Remember, seeking professional medical advice is paramount, and open communication with your pediatrician or specialist is crucial throughout the process.
With the right information and support, you can confidently navigate this journey towards a healthy head shape for your little one.
Quick FAQs
What is the long-term outlook for children with plagiocephaly?
The long-term outlook depends on the type and severity of plagiocephaly. Positional plagiocephaly usually resolves well with treatment. Deformational plagiocephaly often improves significantly with treatment, but some residual asymmetry might remain. Synostotic plagiocephaly requires surgery, and the outcome depends on the extent of the craniosynostosis and the success of the surgery. In most cases, the long-term effects on brain development are minimal, although some children may experience cosmetic concerns.
Are there any long-term cosmetic effects?
While treatment is often very effective, some residual asymmetry may remain in cases of deformational plagiocephaly. The extent of any cosmetic effect varies depending on the severity of the condition and the success of treatment. In many cases, the residual asymmetry is minimal and not noticeable.
Can plagiocephaly affect a child’s intelligence or development?
In most cases, plagiocephaly does not affect a child’s intelligence or overall development. However, in cases of severe craniosynostosis (synostotic plagiocephaly), there’s a potential for increased intracranial pressure which could impact development. Early diagnosis and treatment significantly minimize this risk.