
Why Healthcare Needs Comprehensive Cloud Security
Why the healthcare industry needs a comprehensive cloud security platform is a question increasingly critical in our digitally driven world. The sensitive nature of patient data (PHI), coupled with the rising sophistication of cyberattacks, creates a perfect storm of risk. This isn’t just about protecting financial assets; it’s about safeguarding the well-being and trust of patients. A robust cloud security platform isn’t a luxury – it’s a necessity for survival in today’s threat landscape.
From ransomware attacks crippling hospital systems to phishing scams targeting unsuspecting employees, the challenges are immense. Meeting stringent regulatory requirements like HIPAA and GDPR adds another layer of complexity. However, a well-designed cloud security platform offers a proactive, scalable, and cost-effective solution to these challenges, providing enhanced data visibility, improved control, and stronger compliance.
The Growing Threat Landscape in Healthcare: Why The Healthcare Industry Needs A Comprehensive Cloud Security Platform
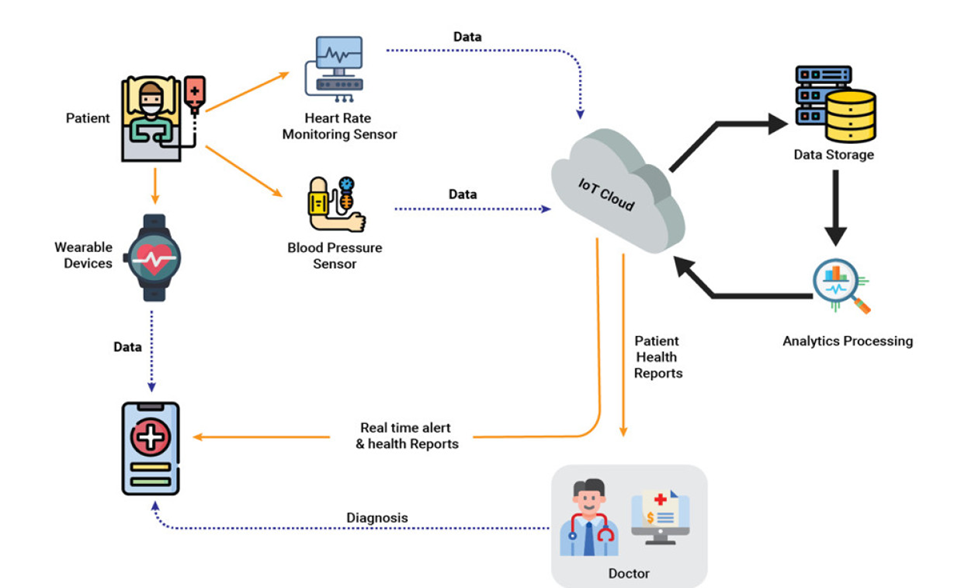
The healthcare industry, a sector entrusted with incredibly sensitive personal information and critical infrastructure, faces an ever-evolving and increasingly sophisticated threat landscape. The convergence of valuable data, interconnected systems, and often legacy technology creates a perfect storm for cybercriminals. This necessitates a robust and comprehensive cloud security platform to mitigate the growing risks.The vulnerabilities within healthcare data are significant.
Patient health information (PHI), including medical records, insurance details, and genetic information, is incredibly valuable on the dark web. A breach can lead to identity theft, financial fraud, and reputational damage for both the patient and the healthcare provider. Moreover, the disruption of critical healthcare systems can have life-threatening consequences. The interconnected nature of modern healthcare, with electronic health records (EHRs), medical devices, and administrative systems all linked, means a single point of compromise can have cascading effects.
Types of Cyberattacks in Healthcare, Why the healthcare industry needs a comprehensive cloud security platform
Healthcare organizations are targeted by a wide range of cyberattacks. Ransomware attacks, which encrypt critical data and demand a ransom for its release, are particularly devastating. These attacks can cripple operations, preventing access to patient records and delaying or preventing crucial medical treatments. Phishing attacks, often disguised as legitimate communications, trick employees into revealing sensitive credentials, providing a gateway for attackers to infiltrate systems.
With sensitive patient data increasingly stored in the cloud, a robust security platform is crucial for the healthcare industry. The recent Supreme Court decision, as reported in scotus overturns chevron doctrine healthcare , highlights the need for clear legal frameworks around data protection, further emphasizing the importance of proactive, comprehensive cloud security measures to safeguard patient privacy and comply with evolving regulations.
This is why investing in a top-notch cloud security platform isn’t just a good idea – it’s a necessity.
Denial-of-service (DoS) attacks overwhelm systems, making them unavailable to legitimate users, which can disrupt essential services. Insider threats, malicious or negligent actions by employees with access to sensitive data, also pose a considerable risk. Advanced Persistent Threats (APTs), sophisticated and long-term attacks often sponsored by nation-states, are becoming increasingly common, aiming to steal valuable intellectual property or sensitive patient data.
The impact of these attacks ranges from financial losses and operational disruptions to reputational damage and legal repercussions.
Financial and Reputational Costs of Data Breaches
The cost of a data breach in healthcare is substantial, encompassing both direct financial losses and indirect reputational damage. The financial costs can include legal fees, regulatory fines, credit monitoring services for affected patients, and the cost of remediation and recovery. Reputational damage can lead to loss of patients, decreased investor confidence, and difficulty in attracting and retaining qualified staff.
| Type of Breach | Cost (USD) | Impact on Operations | Impact on Reputation |
|---|---|---|---|
| Ransomware Attack | $1M – $10M+ (depending on size and recovery time) | System downtime, delayed treatments, loss of patient data | Loss of patient trust, negative media coverage, decreased investor confidence |
| Phishing Attack leading to data theft | $100,000 – $500,000+ (depending on data compromised) | Potential disruption of services, investigation costs | Damage to credibility, loss of patient trust, potential legal action |
| Insider Threat | Variable, potentially very high | Data loss, operational disruption, potential legal action | Severe reputational damage, loss of patient trust |
| DoS Attack | $50,000 – $1M+ (depending on duration and impact) | Significant service disruption, potential loss of revenue | Negative perception of security capabilities |
Benefits of a Cloud-Based Security Approach
Source: globalsign.com
Migrating healthcare security to the cloud offers significant advantages over traditional on-premise systems. The inherent scalability, cost-effectiveness, and enhanced accessibility of cloud-based security platforms are transforming how healthcare organizations protect sensitive patient data. This shift allows for a more proactive and comprehensive approach to cybersecurity, ultimately strengthening the overall security posture.The advantages of a cloud-based approach stem from its inherent flexibility and the resources offered by cloud providers.
Unlike on-premise solutions, which require significant upfront investment in hardware, software, and IT personnel, cloud platforms offer a pay-as-you-go model, reducing capital expenditure and allowing for easier scalability to meet fluctuating demands. This is particularly beneficial for healthcare organizations experiencing rapid growth or seasonal peaks in patient volume. Furthermore, cloud-based solutions often provide access to cutting-edge security technologies and expertise that may be beyond the reach of individual healthcare providers.
Improved Data Visibility and Control
Cloud security platforms offer centralized management and monitoring capabilities, providing a unified view of security events across disparate healthcare settings. This enhanced visibility allows for quicker identification and response to threats, minimizing the impact of potential breaches. For example, a hospital system with multiple clinics can use a cloud platform to monitor access controls, data activity, and security alerts from all locations through a single dashboard.
This level of centralized control allows for the consistent application of security policies and procedures, ensuring compliance with regulations such as HIPAA. Imagine a scenario where a suspicious login attempt is detected at a remote clinic – the cloud platform immediately alerts the security team, enabling swift intervention and prevention of a potential breach. This level of real-time monitoring and response is simply not achievable with disparate, on-premise systems.
Successful Implementations of Cloud Security Platforms
Several healthcare organizations have successfully leveraged cloud security platforms to enhance their security posture. For example, a large hospital system reported a significant reduction in security incidents after implementing a cloud-based security information and event management (SIEM) system. The centralized logging and analysis capabilities of the SIEM allowed them to identify and address vulnerabilities much faster than with their previous on-premise system.
Another case study involves a national telehealth provider that improved its data protection by migrating its sensitive patient data to a cloud platform with robust encryption and access controls. This move significantly reduced the risk of data breaches and improved compliance with data privacy regulations. These successes demonstrate the tangible benefits of embracing cloud-based security solutions in healthcare.
Key Features of a Comprehensive Cloud Security Platform
A robust cloud security platform for healthcare should incorporate several essential features to effectively protect sensitive patient data. These features are critical for maintaining compliance and mitigating risks in the ever-evolving threat landscape.
- Data Loss Prevention (DLP): Preventing sensitive data from leaving the organization’s control through various means, including email, cloud storage, and external devices.
- Intrusion Detection and Prevention Systems (IDPS): Monitoring network traffic for malicious activity and automatically blocking or mitigating threats.
- Access Control and Identity Management: Implementing robust authentication and authorization mechanisms to restrict access to sensitive data based on roles and privileges.
- Data Encryption: Protecting data both in transit and at rest using strong encryption algorithms.
- Security Information and Event Management (SIEM): Centralized logging and analysis of security events to detect and respond to threats.
- Vulnerability Management: Regularly scanning for and remediating security vulnerabilities in systems and applications.
- Cloud Security Posture Management (CSPM): Continuously monitoring the security configuration of cloud environments to ensure compliance with security best practices.
- Threat Intelligence: Leveraging threat intelligence feeds to proactively identify and mitigate emerging threats.
Integrating Cloud Security into Existing Infrastructure
Integrating a cloud security platform into an existing healthcare IT infrastructure presents unique challenges. The complexity stems from the diverse range of systems, often including legacy applications and disparate technologies, all needing to seamlessly communicate and share data while adhering to strict security and privacy regulations like HIPAA. Successfully navigating this requires careful planning, a phased approach, and a deep understanding of both cloud security best practices and the specific nuances of the healthcare environment.
The process demands a holistic view, addressing not just the technological aspects but also the organizational, procedural, and human elements crucial for a secure and effective transition. This involves a careful assessment of current infrastructure, identifying vulnerabilities, and developing a comprehensive migration strategy that minimizes disruption and maximizes security.
With the increasing reliance on cloud technology in healthcare, robust security is paramount. The sensitive nature of patient data demands it, especially considering groundbreaking advancements like the recent FDA approval of clinical trials for pig kidney transplants in humans, as reported here: fda approves clinical trials for pig kidney transplants in humans. This kind of research generates massive amounts of data, highlighting the urgent need for a comprehensive cloud security platform to protect patient privacy and research integrity.
Challenges of Integrating Cloud Security with Existing Infrastructure
Healthcare organizations often grapple with a heterogeneous IT landscape, encompassing legacy systems, various applications, and diverse data formats. Integrating a cloud security platform requires addressing interoperability issues, ensuring seamless communication and data exchange between the new platform and existing systems. Legacy systems, in particular, may lack the necessary security features or APIs for easy integration, requiring careful planning and potentially custom solutions.
Furthermore, the need to comply with regulations like HIPAA adds another layer of complexity, demanding meticulous attention to data privacy and security throughout the integration process. For example, an older radiology system might not be directly compatible with a modern cloud-based security information and event management (SIEM) system, requiring intermediary software or custom integrations to bridge the gap.
Secure Migration of Sensitive Healthcare Data to the Cloud
Migrating sensitive healthcare data to the cloud requires a robust strategy that prioritizes data encryption and access control. Data encryption, both in transit and at rest, is paramount to protect patient information from unauthorized access. This includes employing strong encryption algorithms and key management practices. Access control mechanisms, such as role-based access control (RBAC) and attribute-based access control (ABAC), ensure that only authorized personnel can access specific data based on their roles and responsibilities.
For instance, a radiologist should only have access to radiology images, not patient financial data. A phased migration approach, starting with less sensitive data and gradually moving to more critical information, minimizes risk and allows for iterative testing and refinement of security measures.
Facilitating Collaboration and Data Sharing While Maintaining Patient Privacy
A cloud security platform can significantly enhance collaboration and data sharing among healthcare providers while adhering to strict privacy regulations. By implementing robust access control mechanisms and encryption protocols, the platform can facilitate secure data exchange between different healthcare organizations, enabling efficient care coordination and improved patient outcomes. For example, a cloud-based platform can allow different hospitals to securely share patient medical records, enabling seamless transitions of care and preventing unnecessary duplication of tests.
Protecting sensitive patient data is paramount, making a robust cloud security platform essential for the healthcare industry. This is especially crucial considering the complexities of managing diverse data sets, like understanding nutritional needs – check out this interesting article on how dietary needs differ between genders: are women and men receptive of different types of food and game changing superfoods for women – which highlights the importance of personalized data handling.
Ultimately, a comprehensive security system safeguards patient privacy and ensures the integrity of vital health information.
This requires careful consideration of data anonymization and de-identification techniques to protect patient privacy while still allowing for meaningful data analysis and collaboration.
Step-by-Step Guide to Implementing a Cloud Security Platform
Implementing a cloud security platform in a healthcare organization is a multi-stage process requiring careful planning and execution.
- Assessment and Planning:
Conduct a thorough assessment of the existing IT infrastructure, identifying security gaps and vulnerabilities. Develop a comprehensive plan outlining the migration strategy, timeline, and budget. Consider the impact on various departments and stakeholders.
- Selection and Procurement:
Choose a cloud security platform that aligns with the organization’s specific needs and regulatory requirements. Carefully evaluate different vendors and their offerings, focusing on features like data encryption, access control, threat detection, and compliance certifications.
- Integration and Configuration:
Integrate the chosen platform with existing systems, ensuring seamless data exchange and interoperability. Configure the platform to meet the organization’s specific security policies and regulatory requirements. This may involve custom scripting or API integrations.
- Data Migration:
Develop a phased data migration plan, starting with less sensitive data. Employ robust encryption and access control mechanisms throughout the migration process. Regularly monitor the migration for errors and security breaches.
- Testing and Validation:
Thoroughly test the integrated platform to ensure its effectiveness and identify any potential vulnerabilities. Validate the platform’s compliance with relevant regulations, such as HIPAA. Conduct penetration testing to identify any security weaknesses.
- Monitoring and Maintenance:
Continuously monitor the platform for security threats and vulnerabilities. Implement regular security updates and patches to address any identified issues. Establish clear procedures for incident response and remediation.
Addressing the Human Element in Security

Source: astera.com
Let’s face it: even the most sophisticated cloud security platform is only as strong as the people who use it. In healthcare, where sensitive patient data is constantly being accessed and shared, human error remains a significant vulnerability. Addressing this human element is crucial for building a truly robust security posture. This isn’t about blaming individuals; it’s about recognizing that humans are fallible and implementing strategies to minimize the impact of those fallibilities.The reality is that many healthcare data breaches stem from unintentional actions like clicking on phishing links, falling for social engineering tactics, or simply forgetting to log out of a system.
These seemingly small mistakes can have catastrophic consequences, leading to significant financial penalties, reputational damage, and, most importantly, the compromise of patient trust. Therefore, a comprehensive approach to cybersecurity must include a robust strategy for mitigating human risk.
Security Awareness Training Programs
Effective security awareness training is not a one-time event; it’s an ongoing process. Training should be tailored to the specific roles and responsibilities of healthcare professionals, focusing on the types of threats they are most likely to encounter. This requires a multi-faceted approach that combines engaging modules, interactive exercises, and regular reinforcement. The goal is to foster a security-conscious culture where employees understand the importance of their role in protecting patient data and are empowered to report suspicious activity.
Robust Security Policies and Procedures
Clear, concise, and consistently enforced security policies and procedures are the backbone of any effective security program. These policies should cover all aspects of data security, from access control and password management to incident response and data breach notification. Access control should be based on the principle of least privilege, meaning that employees only have access to the information they need to perform their jobs.
A well-defined incident response plan should Artikel the steps to be taken in the event of a security incident, ensuring a swift and effective response to minimize damage.
Best Practices for Employee Training and Education
Implementing effective training requires a multifaceted approach. This should include regular updates on emerging threats, interactive simulations that mimic real-world scenarios, and opportunities for employees to ask questions and receive clarification. Furthermore, incorporating gamification elements, such as quizzes and rewards, can significantly improve engagement and knowledge retention. The training program should be regularly reviewed and updated to reflect changes in the threat landscape and best practices.
The ultimate goal is to cultivate a culture of vigilance and responsibility, where employees actively participate in protecting sensitive data.
Examples of Effective Security Awareness Campaigns
To make security training engaging and memorable, healthcare organizations can adopt creative strategies. Here are some examples of effective security awareness campaigns:
- Interactive phishing simulations: These simulations expose employees to realistic phishing attempts, allowing them to practice identifying and reporting suspicious emails. The feedback provided after the simulation reinforces learning and highlights areas for improvement.
- Scenario-based training modules: These modules present employees with real-world scenarios involving data breaches and security incidents, allowing them to learn from mistakes and practice their response skills. For instance, a module might simulate a ransomware attack and guide employees through the steps to take to mitigate the damage.
- Gamified security awareness quizzes: Turning security training into a game can significantly boost engagement and knowledge retention. Quizzes can be used to test employees’ understanding of security policies and procedures, with rewards offered for high scores. This makes learning fun and encourages active participation.
- Regular security newsletters and communications: Keeping employees informed about current cybersecurity threats and best practices through regular newsletters and communications is crucial. These updates should highlight recent incidents, provide tips for staying safe online, and remind employees of their responsibilities in protecting patient data. Examples could include real-world case studies of data breaches caused by human error and how those breaches could have been avoided.
Closure
Source: prodwaregroup.com
In conclusion, the healthcare industry faces unprecedented cybersecurity threats, demanding a robust and comprehensive approach to data protection. A cloud-based security platform is no longer optional; it’s the cornerstone of a secure and compliant healthcare ecosystem. By embracing a proactive strategy that integrates advanced security measures, robust compliance frameworks, and a strong focus on employee training, healthcare organizations can effectively mitigate risks, protect sensitive patient information, and maintain the trust of their patients and stakeholders.
The future of healthcare security hinges on this crucial shift towards a more secure digital infrastructure.
Essential FAQs
What are the biggest risks to healthcare data in the cloud?
The biggest risks include data breaches from ransomware, phishing attacks, insider threats, and misconfigurations. These can lead to financial penalties, reputational damage, and loss of patient trust.
How does a cloud security platform help with HIPAA compliance?
A comprehensive platform helps by providing tools for access control, data encryption, audit trails, and vulnerability management, all essential for meeting HIPAA’s stringent requirements.
What are the key features of a good healthcare cloud security platform?
Key features include data loss prevention (DLP), intrusion detection and prevention systems (IDS/IPS), multi-factor authentication (MFA), encryption at rest and in transit, and robust access control mechanisms.
Can a cloud security platform integrate with legacy systems?
Yes, but integration can be complex. Careful planning and potentially phased migration are crucial for seamless integration with existing infrastructure.



