Physician Compensation Climbs Inflation & MGMA Survey
Physician compensation climbs inflation mgmaa surve: The medical field is buzzing! Recent data from the MGMA (Medical Group Management Association) reveals a significant surge in physician compensation, outpacing inflation in many specialties. This isn’t just good news for doctors; it reflects broader trends in the healthcare landscape, impacting everything from access to care to the future of medical practice.
This post delves into the MGMA’s findings, exploring the factors driving these salary increases, the impact of inflation, and what these trends mean for the future of medicine.
We’ll unpack the MGMA survey methodology, examining its strengths and limitations, and comparing its data with other sources. We’ll also explore how compensation varies geographically, across different practice models (solo, group, hospital), and among various specialties. Finally, we’ll look ahead, forecasting potential future trends and challenges based on factors like technological advancements, healthcare policy changes, and the ever-growing impact of telehealth.
Physician Compensation Trends
Source: mgma.com
Physician compensation has seen significant fluctuations over the past decade, influenced by a complex interplay of market forces, healthcare policy changes, and the evolving nature of medical practice. Understanding these trends is crucial for both physicians navigating their careers and healthcare organizations managing their budgets. This analysis will explore the historical trajectory of physician salaries, the factors driving recent increases, and the variations across different medical specialties.Physician Compensation in the Past DecadeThe past decade has witnessed a period of both growth and instability in physician compensation.
While overall compensation has generally trended upwards, the rate of growth has varied considerably year to year, influenced by factors such as the economic climate, changes in healthcare reimbursement models, and the increasing demand for certain specialties. Early in the decade, salary increases were more modest, often lagging behind inflation. However, more recently, we’ve seen a notable acceleration, particularly in certain high-demand specialties.
This surge can be partly attributed to the increasing pressure on the healthcare system, coupled with the growing shortage of physicians in many areas.Factors Contributing to Recent Increases in Physician SalariesThe recent increase in physician salaries, as reflected in data from the Medical Group Management Association (MGMA), is a multifaceted phenomenon. Several key factors are at play: the increasing complexity of medical care, the rising cost of medical education and training, the growing demand for specialists, and the competitive landscape for attracting and retaining qualified physicians.
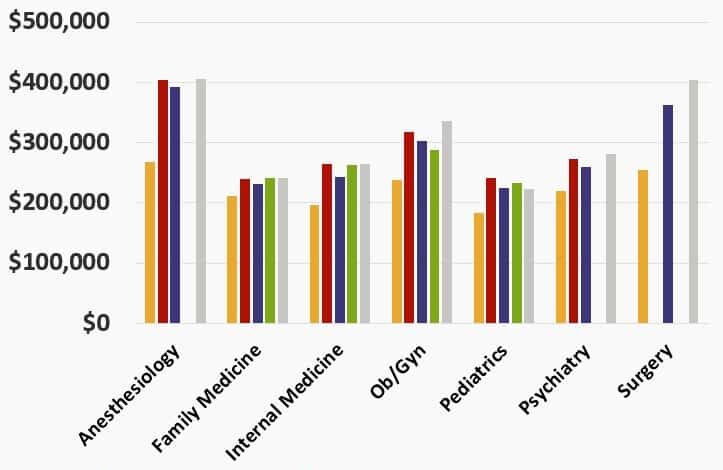
The MGMA data highlights a significant correlation between the shortage of physicians in certain specialties and the corresponding increase in compensation offered to attract and retain qualified individuals. Furthermore, the increasing administrative burden placed on physicians, alongside the growing complexity of electronic health records (EHR) systems, contributes to the need for higher compensation to offset these additional demands on their time and expertise.Physician Compensation Across SpecialtiesThe following table illustrates the significant variation in average compensation across different medical specialties.
So, physician compensation is climbing faster than inflation, according to the MGMA survey – a trend that impacts healthcare access, especially for conditions like dementia. It’s fascinating to consider that early detection might be possible through simple eye tests, as this article suggests: can eye test detect dementia risk in older adults. This could significantly impact the demand for specialists and further influence those physician compensation numbers, wouldn’t you think?
It is important to note that these figures represent averages and can vary widely based on factors such as geographic location, practice setting (e.g., private practice versus hospital employment), and years of experience.
| Specialty | Average Compensation | Compensation Growth Rate (Year-over-Year) | Factors Influencing Compensation |
|---|---|---|---|
| Cardiology | $500,000 – $700,000 (estimated) | 3-5% (estimated) | High demand, complex procedures, significant malpractice risk |
| Orthopedic Surgery | $550,000 – $800,000 (estimated) | 4-6% (estimated) | High demand, surgical expertise, significant procedural volume |
| Dermatology | $350,000 – $550,000 (estimated) | 2-4% (estimated) | High demand, procedural and cosmetic procedures, relatively lower malpractice risk |
| Family Medicine | $200,000 – $350,000 (estimated) | 1-3% (estimated) | High patient volume, broader scope of practice, lower procedural intensity |
Note: The compensation figures and growth rates presented above are estimates based on publicly available data and should be considered approximate. Actual compensation will vary based on numerous factors. The MGMA regularly publishes more detailed and precise compensation data, which should be consulted for the most current and accurate information.
Inflation’s Impact on Physician Earnings
Inflation significantly erodes the purchasing power of physician earnings, impacting their financial well-being in various ways. While physician salaries often see increases, these increases may not always keep pace with the rising cost of living, leaving many doctors struggling to maintain their previous standard of living. Understanding this dynamic is crucial for physicians to effectively manage their finances and advocate for fair compensation.Inflation affects physician purchasing power by reducing the amount of goods and services that can be bought with a given salary.
If inflation rises faster than a physician’s salary, their real income (adjusted for inflation) decreases. This means that despite an apparent salary increase, they can afford less than before. This effect is amplified by the high cost of medical education and the significant financial investment many physicians make in their careers.
The Relationship Between Inflation Rates and Physician Salary Adjustments
The relationship between inflation rates and physician salary adjustments is complex and often lags. Salary negotiations frequently occur annually or less frequently, meaning that physician compensation might not immediately reflect current inflation rates. Furthermore, salary adjustments are often influenced by factors beyond inflation, including market demand for specific specialties, geographic location, and the financial performance of the employing institution (hospital, clinic, or private practice).
For instance, a hospital system facing budget constraints might offer smaller salary increases than a thriving private practice in a high-demand area, even in the face of high inflation. This lag can create a substantial gap between a physician’s income and the actual cost of maintaining their lifestyle and professional expenses.
Inflation’s Impact on Practice Expenses
Inflation directly impacts a physician’s practice expenses, whether they are employed or self-employed. Rising costs of medical supplies, equipment, staffing, and rent significantly reduce the profitability of a practice. For example, a 5% inflation rate could translate to a substantial increase in the cost of pharmaceuticals or medical devices, eating into a practice’s profit margin. Similarly, increasing insurance premiums for malpractice coverage represent a significant and often unpredictable cost for physicians.
For physicians in private practice, these escalating costs can lead to reduced income or necessitate raising patient fees, potentially affecting patient access to care.
Inflation’s Impact on Personal Spending
Inflation affects a physician’s personal spending in much the same way it impacts everyone else. The rising costs of housing, groceries, transportation, and education significantly reduce disposable income. For example, a physician who purchased a home several years ago might find their mortgage payments represent a larger portion of their income as housing costs inflate. Similarly, the cost of educating children, a significant expense for many families, increases substantially with inflation.
These inflationary pressures on personal spending can force physicians to make difficult choices about lifestyle, savings, and investments, potentially delaying retirement plans or limiting charitable contributions.
MGMA Survey Methodology and Data
Source: lookforzebras.com
The Medical Group Management Association (MGMA) conducts annual compensation surveys providing valuable insights into physician salaries and benefits. Understanding their methodology and potential limitations is crucial for interpreting the data accurately. This section delves into the MGMA’s approach, highlighting potential biases, and comparing their findings with data from other sources.The MGMA’s physician compensation surveys rely on a robust data collection process.
They collect data through a voluntary online survey distributed to their member organizations, encompassing a wide range of medical specialties and practice settings. Participants provide detailed information on physician compensation, including base salary, bonuses, benefits, and other forms of compensation. The data is then analyzed and aggregated to produce average compensation figures, often broken down by specialty, geographic location, practice size, and other relevant factors.
Statistical methods are used to account for variations in data and to produce reliable estimates. Weighting techniques may be applied to ensure the sample is representative of the broader physician population. However, it is important to note that the final figures represent averages and should be considered estimates rather than precise measurements for any given physician.
MGMA Survey Methodology Details
The MGMA employs a stratified random sampling technique to select participants for its survey. This approach aims to ensure representation across different specialties, practice sizes, and geographic regions. Data is collected using online questionnaires, allowing for efficient data collection and analysis. Data cleaning and validation procedures are implemented to identify and address any inconsistencies or errors. The final data set is rigorously analyzed to generate compensation benchmarks.
The specific statistical methods employed may vary from year to year, and detailed descriptions are usually available in the full survey reports. The MGMA emphasizes the importance of a large and diverse sample size to enhance the reliability and generalizability of the findings. However, it’s crucial to acknowledge that the participation rate in such voluntary surveys is always less than 100%.
Limitations and Biases in MGMA Data
While the MGMA strives for comprehensive data collection, several limitations and potential biases should be considered when interpreting their results. The voluntary nature of the survey introduces a potential for selection bias. Physicians who choose to participate may differ systematically from those who do not, leading to an unrepresentative sample. For example, practices with higher compensation might be more likely to participate, potentially inflating the average compensation figures.
Furthermore, the data primarily reflects compensation in MGMA member practices, which may not perfectly represent all physician practices across the nation. The data might also underrepresent smaller practices or those in underserved areas, potentially skewing the overall averages. Another potential bias could stem from variations in reporting practices among participants. Inconsistent reporting of benefits or other compensation components can affect the accuracy of the overall compensation figures.
Finally, the survey relies on self-reported data, which can be subject to recall bias or intentional misreporting.
Comparison with Other Compensation Data Sources
Several other organizations and companies also collect and publish physician compensation data. Comparing the MGMA data with these alternative sources can provide a more comprehensive understanding of physician earnings. Direct comparison can be challenging due to differences in methodology, sample populations, and data collection periods. However, a general overview can highlight areas of agreement and discrepancy.
| Data Source | Average Compensation | Methodology | Key Differences from MGMA |
|---|---|---|---|
| MGMA | Varies by specialty, location, and practice size (Specific figures are not provided here due to their variability and the need for reference to the actual MGMA reports) | Voluntary online survey; stratified random sampling | Focuses on MGMA member practices; potential for selection bias |
| Physician Compensation Report (Example – hypothetical data for illustrative purposes only) | (Hypothetical average: $300,000) | Analysis of publicly available data from various sources; proprietary algorithms | Wider data sources; different weighting and aggregation techniques; may include non-MGMA member practices |
| [Another Data Source – Example – hypothetical data for illustrative purposes only] | (Hypothetical average: $280,000) | National survey of physicians; stratified sampling; weighted averages | Larger sample size; different geographic coverage; potentially different weighting strategies; different data collection period. |
Geographic Variations in Physician Compensation
Physician compensation in the United States isn’t uniform; significant regional disparities exist, impacting the financial well-being and career choices of physicians across the country. These variations stem from a complex interplay of factors, making understanding these differences crucial for both physicians and healthcare organizations.The most recent MGMA data reveals substantial salary discrepancies between different geographic regions. For example, specialists in major metropolitan areas on the coasts often command significantly higher salaries than their counterparts in rural areas of the Midwest or South.
These differences aren’t simply about the prestige of location; they are rooted in a number of interconnected economic and market forces.
Factors Contributing to Geographic Variation in Physician Compensation, Physician compensation climbs inflation mgmaa surve
Several key factors influence the significant regional variations observed in physician salaries. These include cost of living, market demand for specific specialties, the prevalence of healthcare regulations, and the overall economic health of the region.Cost of living plays a significant role. High-cost-of-living areas, such as major cities on the coasts, typically require higher salaries to attract and retain qualified physicians.
These areas often have higher housing costs, taxes, and everyday expenses, necessitating compensation adjustments to maintain a comparable standard of living.Market demand for specific specialties also creates variations. Areas with a shortage of specialists, such as cardiologists in rural communities or oncologists in underserved urban areas, often offer higher salaries to incentivize recruitment. Conversely, areas with a surplus of a particular specialty may see lower compensation rates due to increased competition.Healthcare regulations and reimbursement policies also influence physician compensation.
States with stricter regulations or lower reimbursement rates for certain procedures may result in lower physician salaries. Conversely, states with more favorable regulatory environments or higher reimbursement rates may attract physicians and offer higher compensation. Finally, the overall economic health of a region influences physician compensation. Regions with robust economies and higher overall incomes tend to offer higher physician salaries.
So, physician compensation is climbing faster than inflation, according to the MGMA survey – a trend partly driven by increased administrative burdens. A big part of that burden is medical coding, and finding qualified coders is a huge challenge. That’s why I was interested to read about the ai powered solution to the medical coding worker shortage , which could potentially free up physicians’ time and ultimately impact those compensation figures.
Less time spent on admin means more time seeing patients, right? Hopefully, this AI solution helps address the current staffing crisis and contributes to a more sustainable model for physician compensation in the long run.
Illustrative Map of Regional Compensation Differences
Imagine a map of the contiguous United States. The coastal regions, particularly along the East and West Coasts, are depicted in shades of deep red and orange, representing the highest physician compensation levels. Major metropolitan areas like New York City, Boston, Los Angeles, and San Francisco are particularly vibrant, indicating extremely high salaries for many specialties. These areas reflect the high cost of living and intense competition for skilled physicians.In contrast, the central and southern regions of the country are shown in lighter shades of orange, yellow, and even green, indicating lower average physician compensation.
Rural areas within these regions appear in a paler green, signifying the lowest compensation levels. For instance, parts of the Midwest and the South, especially rural areas, show significantly lower compensation due to factors like lower cost of living, reduced demand for certain specialties, and potentially lower reimbursement rates. The map visually emphasizes the stark contrast between high-paying urban centers and lower-paying rural areas.
The variations are not uniform across all specialties; some specialties, like primary care, may exhibit less pronounced regional disparities than high-demand surgical subspecialties.
Physician Compensation and Practice Models
Choosing a practice model significantly impacts a physician’s compensation and overall career trajectory. The traditional solo practice is becoming increasingly rare, while group practices and hospital employment are dominant forces shaping the compensation landscape. Understanding the nuances of each model is crucial for physicians navigating their career paths.The compensation structure within each practice model varies considerably, influenced by factors such as specialty, location, productivity, and the specific contractual agreements in place.
While some models offer greater autonomy, others provide enhanced benefits and stability. Let’s delve into the specifics of each model and their associated compensation structures.
Solo Practice Compensation
Solo practitioners typically receive 100% of their collected revenue after deducting expenses. This offers maximum earning potential, but also carries the full burden of overhead costs, including rent, staff salaries, insurance, and malpractice premiums. Income is directly tied to patient volume and efficiency, creating significant financial risk and requiring robust business acumen beyond clinical skills. Many physicians find the administrative burden overwhelming, limiting the time available for patient care.
This model is becoming less common due to the significant financial and administrative challenges involved.
Group Practice Compensation
Group practices offer a more collaborative environment and often feature a compensation model based on a salary plus productivity bonus or a percentage of collections. Overhead costs are shared among the physicians, reducing individual financial risk. However, compensation may be less than in a solo practice if productivity is not high. The collaborative nature can lead to professional growth and shared resources, but individual autonomy can be limited by group policies and decision-making processes.
For example, a cardiologist in a large multi-specialty group might earn a base salary plus a bonus tied to the number of procedures performed, resulting in a compensation that varies based on patient volume and procedural efficiency.
Hospital Employment Compensation
Hospital employment offers a stable salary, benefits package, and reduced administrative burden. Compensation is typically structured as a base salary, often supplemented by bonuses based on performance metrics such as patient satisfaction, quality measures, or adherence to hospital protocols. While this provides financial security and predictable income, it might limit earning potential compared to solo or group practices, particularly for high-volume specialists.
The trade-off is a more predictable income stream with less financial risk and administrative overhead. A radiologist employed by a large hospital system, for instance, may receive a fixed annual salary, potentially with additional compensation for exceeding certain imaging volumes or achieving high patient satisfaction scores.
Physician Employment Pathways and Compensation Structures
The decision of how to enter into a practice setting directly impacts compensation and career trajectory. The following flowchart illustrates common pathways and their associated compensation structures.
So, physician compensation is finally outpacing inflation, according to the MGMA survey – good news for doctors! But this increased revenue also means heightened responsibility, especially concerning data security. Hospitals need to be on top of their game, which is why understanding the hhs healthcare cybersecurity framework hospital requirements cms is crucial. Ultimately, robust cybersecurity protects both patient data and the financial stability of these increasingly lucrative medical practices.
Start
|
V
+-------------------------------------------------+
| Choice |
+-------------------------------------------------+
|
V
+---------------------+ +---------------------+ +---------------------+
| Solo Practice | | Group Practice | | Hospital Employment |
+---------------------+ +---------------------+ +---------------------+
|
V
100% of revenue (after expenses) Salary + Bonus/Percentage of Collections Fixed Salary + Bonuses
|
V
Outcome
The flowchart depicts three primary paths: solo practice, characterized by high risk, high reward; group practice, offering a balance of risk and reward; and hospital employment, providing stability and predictable income but potentially limiting earning potential.
The compensation structure for each path is indicated, highlighting the variability in income and financial responsibility.
Future Projections for Physician Compensation
Source: lookforzebras.com
Predicting the future of physician compensation is a complex undertaking, influenced by a multitude of interconnected factors. While precise figures are impossible, analyzing current trends and foreseeable changes allows us to sketch a plausible picture of what lies ahead for physician earnings. This projection considers the interplay of inflation, technological disruption, evolving healthcare policies, and shifting practice models.
The coming years will likely see continued pressure on physician compensation. Inflation, a persistent economic headwind, will undoubtedly continue to erode the purchasing power of physician salaries. However, the degree of this erosion will depend on the overall economic climate and the effectiveness of government interventions. Simultaneously, technological advancements, while offering opportunities, also present challenges. The rise of telehealth and artificial intelligence could lead to both increased efficiency and decreased demand for certain types of physician services, affecting compensation accordingly.
The Impact of Telehealth and Remote Care on Physician Earnings
Telehealth’s rapid growth presents a double-edged sword for physician compensation. On one hand, it expands access to care, potentially increasing patient volume and revenue for some physicians. Telemedicine platforms can also reduce overhead costs associated with physical office space. However, reimbursement rates for telehealth services are often lower than those for in-person visits, and the increased competition from providers offering remote care could depress overall compensation in some specialties.
For example, a cardiologist specializing in remote monitoring might see a slight increase in patient volume, but lower reimbursement rates per patient could negate the overall benefit. Conversely, a dermatologist primarily reliant on in-person examinations might see a decrease in patient volume as more patients opt for online consultations with lower-cost providers.
Potential Challenges and Opportunities Facing Physicians Regarding Future Compensation
The future of physician compensation hinges on several key factors. Understanding these challenges and opportunities is crucial for physicians to navigate the evolving healthcare landscape effectively.
The following points Artikel potential challenges and opportunities:
- Challenge: Increasing administrative burden and declining reimbursement rates from insurers. Many physicians spend significant time on administrative tasks, reducing time for patient care and impacting overall earnings. Simultaneously, insurers are increasingly tightening reimbursement policies, further impacting profitability.
- Opportunity: Specialization in high-demand areas. Physicians specializing in areas with growing needs, such as geriatrics or oncology, may see increased demand and higher compensation.
- Challenge: Competition from non-physician providers, such as nurse practitioners and physician assistants. The expanding scope of practice for these providers can lead to increased competition for patients and potentially lower physician salaries in certain areas.
- Opportunity: Embracing technological advancements and innovative practice models. Physicians who effectively integrate telehealth, AI, and other technologies into their practices can improve efficiency and potentially increase revenue streams.
- Challenge: Uncertainty surrounding healthcare policy changes. Changes in government regulations, insurance policies, and healthcare funding models can significantly affect physician compensation.
- Opportunity: Developing strong relationships with insurers and negotiating favorable contracts. Physicians who effectively negotiate reimbursement rates with insurance companies can ensure better compensation for their services.
Last Point: Physician Compensation Climbs Inflation Mgmaa Surve
The MGMA survey paints a dynamic picture of physician compensation, highlighting a complex interplay between inflation, market demand, and practice models. While higher salaries are undoubtedly positive for physicians, the data also reveals significant disparities across specialties and geographic locations. Understanding these trends is crucial for both physicians navigating career decisions and policymakers shaping the future of healthcare. The ongoing evolution of the medical field, influenced by technological advancements and shifting healthcare paradigms, ensures that the conversation around physician compensation will remain a vital and evolving one.
Top FAQs
What factors besides inflation influence physician compensation?
Many factors influence physician compensation, including specialty (surgeons generally earn more than family physicians), experience level, location (cost of living and market demand play a role), practice setting (hospital employment often differs from private practice), and productivity.
How does the MGMA survey compare to other compensation data sources?
The MGMA is a widely respected source, but its data may not perfectly reflect every practice or region. Comparing MGMA data with other sources like the American Medical Association (AMA) or independent consulting firms can provide a more holistic view, though methodologies and data collection may vary.
What are the long-term implications of these compensation trends?
Sustained increases in physician compensation could lead to higher healthcare costs, but they may also attract more talented individuals to the profession, potentially improving access to care in underserved areas. The long-term impact will depend on various factors, including government regulations and healthcare market dynamics.