Medicare Advantage Overpayments Inflated Benchmarks, Health Affairs
Medicare advantage overpayments inflated benchmarks health affairs – Medicare Advantage Overpayments: Inflated Benchmarks, Health Affairs – this phrase encapsulates a critical issue facing our healthcare system. A recent Health Affairs article shines a light on how inflated benchmarks in the Medicare Advantage program are leading to significant overpayments, costing taxpayers billions and potentially jeopardizing the long-term solvency of Medicare. This isn’t just about numbers; it’s about the impact on access to care, the fairness of the system, and the future of healthcare for millions of Americans.
We’ll delve into the specifics of this problem, exploring its historical context, the methodology used to uncover the overpayments, and potential solutions to address this critical issue.
The core problem stems from the way Medicare Advantage plans are reimbursed. These plans, which are offered by private companies, receive payments based on benchmarks that, according to the Health Affairs study, are significantly inflated. This inflation leads to excessive payments to these plans, money that could be used to improve other aspects of the Medicare program or reduce the burden on taxpayers.
We’ll examine how risk adjustment models, which are meant to account for the health needs of beneficiaries, play a significant role in these overpayments, and how inaccuracies within these models contribute to the problem.
Medicare Advantage Overpayment Issue Overview
The Medicare Advantage (MA) program, designed to offer seniors alternative health insurance plans to traditional Medicare, has been plagued by concerns regarding significant overpayments. This stems from a complex interplay of factors, primarily the use of inflated benchmarks in calculating the payments made to MA plans. These inflated benchmarks lead to higher payments than what’s justified by the actual cost of providing care to beneficiaries.
The result is a substantial drain on taxpayer dollars and a critical question about the program’s financial sustainability.The current overpayment situation is not a recent development. It’s rooted in the historical evolution of the MA program itself. Initially designed as a cost-effective alternative, the payment methodology has evolved over time, incorporating risk adjustment models intended to fairly compensate plans for the health needs of their beneficiaries.
However, these models, particularly the risk adjustment models used to determine the benchmarks, have been subject to criticism for being susceptible to manipulation and resulting in overestimation of the costs of caring for MA enrollees. This has created a system where plans are incentivized to enroll sicker individuals, leading to higher payments even if the actual cost of care is lower than initially projected.
Types of Medicare Advantage Overpayments
The Health Affairs article highlights several distinct types of overpayments within the MA system. These are not mutually exclusive and often overlap. One major category involves inaccuracies and inconsistencies in the risk adjustment data used to determine payments. This includes issues with coding practices by physicians, where diagnoses are upcoded to reflect higher levels of severity and thus higher payments.
Another significant area of concern relates to the coding of diagnoses for beneficiaries with multiple conditions. The complexity of comorbidity often leads to an overestimation of the cost of care, driving up payments to the MA plans. Finally, there are concerns about the accuracy of the benchmarks themselves, suggesting that the base rates used to calculate payments might be systematically inflated, regardless of the accuracy of the risk adjustment data.
These various mechanisms, operating individually and in concert, contribute to the substantial overpayments observed in the MA program.
Impact of Inflated Benchmarks on Medicare Spending

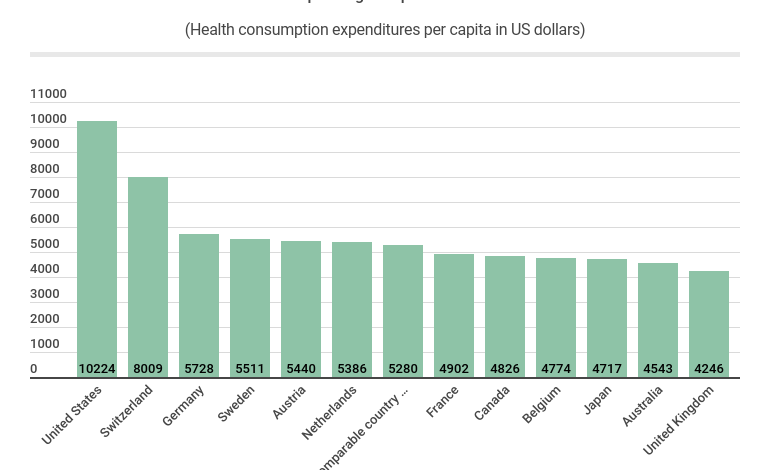
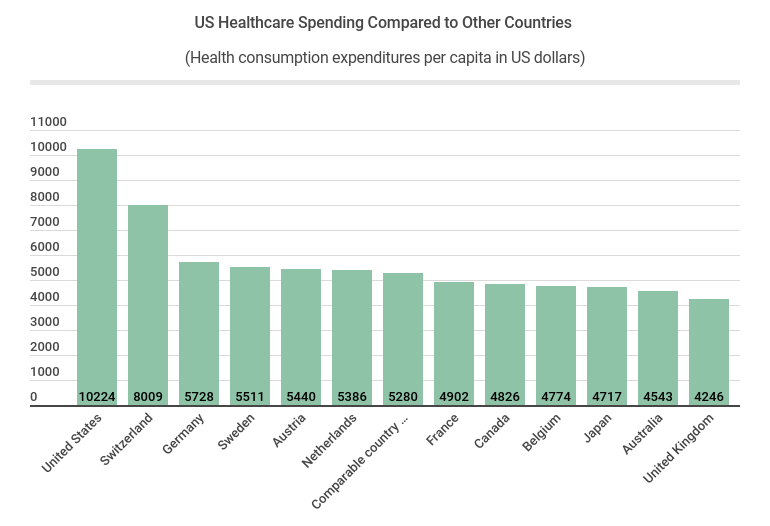
Source: usahealthcare.org
The inflation of benchmarks used in Medicare Advantage (MA) plans has significant financial implications for the Medicare program and, ultimately, American taxpayers. These inflated benchmarks lead to overpayments to MA plans, diverting funds that could be used for other crucial healthcare initiatives or to help keep premiums lower for beneficiaries. Understanding the magnitude of this issue is crucial for ensuring the long-term sustainability of Medicare.The financial implications of inflated benchmarks are multifaceted and far-reaching.
Overpayments to MA plans directly translate to increased Medicare spending. This increased spending is not necessarily reflective of improved quality of care or increased access to services for beneficiaries; rather, it represents a misallocation of taxpayer dollars due to flawed risk adjustment methodologies and potentially fraudulent practices. These overpayments erode the resources available for other essential Medicare programs, potentially impacting beneficiaries’ access to necessary care and services.
Medicare Spending Increases Due to Inflated Benchmarks
The Centers for Medicare & Medicaid Services (CMS) uses a risk adjustment model to determine payments to MA plans based on the health status of their enrollees. However, flaws in this model, along with potential manipulation by MA plans, lead to inflated risk scores and consequently, higher payments. For example, studies have shown that some MA plans have systematically over-reported the severity of their enrollees’ conditions, leading to significantly higher payments than justified by their actual costs.
The cumulative effect of these overpayments across numerous MA plans results in billions of dollars in excess spending annually. This money could have been used for things like expanding access to preventative care, lowering premiums, or improving the quality of care for all Medicare beneficiaries.
Examples of How Overpayments Affect Taxpayer Dollars
Consider a hypothetical scenario: If an MA plan receives an overpayment of $100 per beneficiary due to inflated risk scores, and the plan has 10,000 beneficiaries, the overpayment amounts to $1 million. Multiplied across numerous plans nationwide, these overpayments add up to billions of dollars in wasted taxpayer funds. These funds could have been used to support other crucial government programs or to reduce the national debt.
Moreover, these overpayments ultimately impact taxpayers through higher taxes or reduced funding for other essential public services. Specific examples of this impact can be seen in reports from the Government Accountability Office (GAO) and various journalistic investigations detailing the scale of MA overpayments.
Potential Long-Term Effects on Medicare’s Solvency, Medicare advantage overpayments inflated benchmarks health affairs
The continued inflation of benchmarks in MA poses a serious threat to the long-term solvency of the Medicare program. Sustained overpayments at the current rate are unsustainable and will inevitably lead to a depletion of Medicare’s trust fund. This could result in future benefit cuts, premium increases, or even a crisis in the program’s ability to provide adequate healthcare coverage to the growing elderly population.
The long-term consequences of inaction are potentially severe, demanding urgent action to address the root causes of these overpayments. Failure to correct these issues risks jeopardizing the future of Medicare and the well-being of millions of American seniors.
Analysis of the Health Affairs Article’s Methodology
The Health Affairs article on Medicare Advantage overpayments employs a robust, albeit complex, methodology to arrive at its conclusions. Understanding this methodology is crucial to evaluating the validity and implications of its findings. The authors cleverly combine statistical modeling with detailed analysis of Medicare payment data to quantify the potential for overpayment.The core of the methodology relies on comparing actual Medicare Advantage payments to a counterfactual benchmark.
This benchmark represents what paymentsshould* have been, had the plans adhered strictly to a more efficient and transparent payment structure. The difference between actual payments and the benchmark provides an estimate of the overpayment. Several statistical techniques are used to adjust for factors that might influence spending, ensuring a more accurate comparison.
Benchmark Construction and Refinement
The article’s strength lies in its sophisticated approach to benchmark creation. Instead of using a simple average or historical spending, the authors develop a multi-faceted model that accounts for variations in beneficiary health status, geographic location, and plan characteristics. This reduces the risk of attributing overpayments to legitimate variations in patient needs or plan efficiency. However, a limitation arises from the inherent complexities of modeling such a diverse range of factors.
The model’s assumptions, particularly regarding the weighting of different variables, could influence the final overpayment estimates. Any inaccuracies or biases in the underlying data used to build the model would also propagate through the analysis. Future research might benefit from exploring alternative benchmark construction methods, such as those incorporating machine learning techniques to capture non-linear relationships between variables.
Statistical Techniques Employed
The researchers utilize regression analysis to control for various confounding variables that could skew the results. This helps isolate the effect of potentially inflated benchmarks on Medicare Advantage spending. Specifically, they likely employ techniques like multilevel modeling to account for the nested structure of the data (beneficiaries nested within plans, plans nested within regions). The strength of this approach is its ability to adjust for numerous factors simultaneously, providing a more precise estimate of the overpayment.
However, the limitations stem from the potential for omitted variable bias – factors not included in the model could still influence spending and lead to inaccurate estimates. Additionally, the accuracy of the results hinges on the assumptions made about the functional form of the relationships between variables. A misspecification of these relationships could lead to biased estimates.
The recent Health Affairs study highlighting inflated benchmarks driving Medicare Advantage overpayments is seriously concerning. It makes you wonder if similar accounting practices are happening elsewhere, especially given that NextGen Healthcare, a major player in healthcare IT, is exploring a sale according to Reuters. This raises questions about potential vulnerabilities within the entire system, and how these inflated Medicare Advantage payments might be connected to broader industry pressures.
Comparison with Other Studies
The Health Affairs study’s findings are largely consistent with other research indicating substantial overpayments in the Medicare Advantage program. Several reports from the Centers for Medicare & Medicaid Services (CMS) and independent researchers have documented similar trends of increasing spending in Medicare Advantage relative to traditional Medicare. However, the magnitude of the overpayment varies across studies, likely reflecting differences in methodology, data sources, and time periods.
Some studies may focus on specific aspects of Medicare Advantage spending, such as drug costs or utilization rates, providing a more granular analysis than the Health Affairs study’s broader approach. Direct comparisons across studies require careful consideration of these methodological differences. Further research synthesizing findings across multiple studies, using meta-analytic techniques, could help to refine the overall understanding of Medicare Advantage overpayments and their drivers.
Role of Risk Adjustment in Medicare Advantage Overpayments
Source: amazonaws.com
Medicare Advantage (MA) plans receive payments from the government based on the health status of their enrollees. A crucial component of this payment system is risk adjustment, a process designed to ensure that plans are fairly compensated for the higher costs associated with caring for sicker individuals. However, flaws in this system have contributed significantly to the overpayments observed in recent years.Risk adjustment uses statistical models to predict the healthcare costs of individuals based on their diagnosed conditions and other demographic factors.
These models assign a risk score to each enrollee, with higher scores indicating a greater likelihood of high healthcare costs. MA plans are then paid a per-member, per-month (PMPM) amount based on these risk scores, meaning higher risk scores lead to higher payments. The accuracy of these risk scores is therefore paramount to ensuring fair and efficient allocation of funds.
Inaccuracies in Risk Adjustment Models and Inflated Benchmarks
Inaccuracies in risk adjustment models stem from several sources. One major issue is the potential for coding errors and upcoding—the practice of assigning diagnoses codes that reflect a higher level of severity than is actually warranted. This practice inflates the risk scores, leading to higher payments for MA plans. Another problem is the limitations of the models themselves.
The models may not accurately capture the complexity of individual health conditions or the interaction of multiple conditions. Finally, the data used to build and validate the risk adjustment models may be incomplete or biased, further affecting the accuracy of the risk scores. These inaccuracies cumulatively contribute to inflated benchmarks, creating a system where MA plans are rewarded for artificially inflating the perceived health risks of their enrollees.
Hypothetical Scenario Illustrating the Impact of Risk Adjustment Errors
Consider two hypothetical MA plans, Plan A and Plan B. Both plans have 1,000 enrollees with similar demographics and average health status. However, Plan A engages in aggressive upcoding, resulting in artificially inflated risk scores for many of its enrollees. Plan B, on the other hand, accurately codes its enrollees’ diagnoses. As a result, Plan A receives a significantly higher PMPM payment than Plan B, even though both plans provide comparable levels of care.
Let’s assume Plan B receives a PMPM payment of $1,000, reflecting the true cost of caring for its enrollees. Due to upcoding, Plan A receives a PMPM payment of $1,200. Over a year, this difference amounts to an overpayment of $200,000 ($200 x 1,000 enrollees). This simple scenario illustrates how inaccuracies in risk adjustment, even in a relatively small scale, can lead to substantial overpayments to MA plans, ultimately impacting taxpayer dollars and potentially reducing the resources available for other healthcare programs.
Potential Solutions and Policy Recommendations
Addressing the issue of inflated benchmarks in Medicare Advantage requires a multi-pronged approach involving regulatory reform, enhanced data transparency, and improved oversight. Simply put, we need to ensure the system accurately reflects the true cost of care, preventing excessive payments to insurers while protecting beneficiary access to quality healthcare. This requires a careful balancing act.The following table Artikels potential solutions, their anticipated impact, and the challenges in implementing them.
The recent Health Affairs article on inflated Medicare Advantage benchmarks and overpayments really got me thinking. It highlights the urgent need for healthcare reform, especially considering the aha hospital groups’ court brief urging a stay to restore the Affordable Care Act’s preventive services. This legal battle underscores how crucial strong, comprehensive healthcare legislation is to preventing further financial instability within the system, ultimately impacting those same inflated Medicare Advantage payments.
It’s crucial to understand that these are not mutually exclusive and a combination of strategies will likely be necessary for effective reform.
| Solution | Potential Impact | Challenges to Implementation |
|---|---|---|
| Refine Risk Adjustment Methodology: Improve the accuracy of the risk adjustment models used to determine payments, reducing reliance on potentially inflated factors. This could involve incorporating more granular data on patient conditions, utilizing more sophisticated statistical modeling techniques, and regularly auditing the accuracy of the models. | Reduced overpayments, more accurate reflection of actual healthcare costs, potentially leading to savings for Medicare. | Requires significant investment in data collection and analysis, ongoing monitoring and evaluation of the models, and potential resistance from MA plans who may benefit from the current system. Developing more sophisticated models is a complex technical undertaking. |
| Strengthen Oversight and Auditing: Increase the frequency and intensity of audits of Medicare Advantage plans to detect and address fraudulent or abusive billing practices. This includes strengthening the Centers for Medicare & Medicaid Services (CMS) capacity for data analysis and investigation. | Reduced overpayments due to fraud and abuse, improved accountability of MA plans. | Requires increased resources for CMS, potential challenges in detecting sophisticated schemes, and the need for robust legal frameworks to prosecute offenders. Auditing is a resource-intensive process. |
| Increase Transparency and Data Sharing: Enhance public access to Medicare Advantage payment data, allowing researchers, policymakers, and the public to scrutinize payment patterns and identify potential areas of concern. This could involve more readily available and easily interpretable data sets. | Increased public awareness of the issue, potential for greater scrutiny and pressure on MA plans to improve their billing practices, fostering a more competitive market. | Concerns about protecting the privacy of beneficiary data, potential for misinterpretation of complex data by the public, and the need for clear and accessible data visualization tools. |
| Implement a More Robust Benchmarking System: Develop a more accurate and reliable system for establishing benchmarks, potentially using a combination of methods including historical data, claims data, and cost reports from a broader range of providers, including non-MA plans. | More accurate cost estimations, reduced overpayments, improved fairness in reimbursement rates. | Requires extensive data collection and analysis, potentially significant upfront investment, and the need to address potential biases in the data used to develop benchmarks. Establishing a consensus on the best methodology will be challenging. |
Regulatory Actions to Mitigate Overpayments
Examples of regulatory actions include imposing stricter penalties for fraudulent billing practices, implementing stricter requirements for data reporting by MA plans, and increasing the resources allocated to CMS for oversight and enforcement. For instance, CMS could issue clearer guidelines on appropriate coding practices, increasing the scrutiny of outlier payments, and potentially imposing financial penalties for non-compliance. This could also include more rigorous review of risk adjustment data submissions by MA plans.
Furthermore, enhanced collaboration between CMS and state insurance regulators could help to identify and address systemic issues.
Comparison of Medicare Advantage and Traditional Medicare
Understanding the differences between Medicare Advantage (MA) and Traditional Medicare (often called Original Medicare) is crucial for beneficiaries navigating the system. Both offer coverage for Medicare-eligible individuals, but their structures, payment models, and beneficiary experiences differ significantly, leading to varying potential for overpayments and cost-sharing.Medicare Advantage and Traditional Medicare utilize fundamentally different payment models. Traditional Medicare operates on a fee-for-service (FFS) basis.
This means that providers are paid separately for each service rendered. Medicare Part A (hospital insurance) covers inpatient care, and Part B (medical insurance) covers physician services, outpatient care, and some preventive services. The beneficiary typically pays a deductible and coinsurance for covered services. In contrast, Medicare Advantage plans are offered by private insurance companies and operate under a capitated payment system.
The insurance company receives a predetermined monthly payment from Medicare per enrollee, regardless of the services rendered. This payment is adjusted based on the health status of the enrollees. This creates incentives for the private plans to manage costs effectively, but also introduces the potential for financial incentives that might conflict with providing the best possible care.
The recent Health Affairs report on inflated Medicare Advantage benchmarks and resulting overpayments got me thinking about healthcare worker burnout. It’s easy to see how flawed systems contribute to the stress that led to the recent new york nurse strike deal reached at Mount Sinai and Montefiore , highlighting the urgent need for systemic reform. Ultimately, fixing the Medicare Advantage overpayment issue is crucial for ensuring fair compensation and sustainable healthcare, which impacts everyone, including nurses.
Payment Models and Overpayment Potential
The fee-for-service model of Traditional Medicare, while seemingly straightforward, has its own vulnerabilities to overpayment. Unnecessary or excessive utilization of services can lead to higher overall spending. Lack of strong oversight and potential for provider-induced demand are contributing factors. While safeguards exist, the potential for overpayments in Traditional Medicare remains a concern. The capitated payment model of Medicare Advantage, while aiming to control costs, presents a different type of overpayment risk.
Inflated risk adjustment scores, as discussed in the Health Affairs article, can lead to plans receiving higher payments than warranted, resulting in significant overpayments. The complexity of the risk adjustment methodology and the potential for manipulation create this vulnerability. The incentive structure inherent in the capitated system means that the plan profits from under-utilization of services as much as from appropriate cost control.
Cost-Sharing and Beneficiary Experiences
Cost-sharing varies significantly between the two programs. Traditional Medicare involves a combination of premiums, deductibles, and coinsurance. Part A has a deductible for each inpatient hospital stay, and Part B has an annual deductible and a 20% coinsurance for most services. Beneficiaries are responsible for paying these out-of-pocket costs. Medicare Advantage plans, on the other hand, offer varying levels of cost-sharing depending on the specific plan.
Some plans offer lower premiums but higher out-of-pocket costs, while others may have higher premiums but lower out-of-pocket expenses. The predictability of costs is often higher with MA plans due to the defined cost-sharing structure within the plan. However, the network restrictions of many MA plans can limit beneficiary choice and potentially lead to higher costs if care is sought outside the network.
Beneficiary experience also differs. Traditional Medicare offers greater choice of providers, but can be more complex to navigate, particularly regarding billing and claims processing. Medicare Advantage plans often provide additional benefits, such as vision, hearing, and dental coverage, but may involve stricter limitations on provider choice and more stringent utilization management processes.
Stakeholder Perspectives on Medicare Advantage Overpayments
The issue of Medicare Advantage overpayments, fueled by inflated benchmarks, doesn’t affect everyone equally. Different stakeholders – beneficiaries, providers, payers (Medicare Advantage plans), and the government – experience the consequences in unique ways, often with conflicting interests. Understanding these diverse perspectives is crucial for developing effective solutions. The impact of inflated benchmarks ripples through the entire healthcare system, affecting access to care, healthcare costs, and the sustainability of the Medicare program itself.
Beneficiary Perspectives on Inflated Benchmarks
Beneficiaries, the ultimate consumers of Medicare services, are indirectly affected by inflated benchmarks. While they might not directly see the overpayments, the consequences can manifest in several ways. Higher premiums, reduced benefits, or even limitations on provider choice can result from the financial strain on Medicare Advantage plans stemming from inflated benchmark costs. These plans may attempt to recoup losses by implementing cost-saving measures that negatively impact beneficiaries’ access to care.
- Increased premiums or reduced benefits due to plan financial pressures.
- Narrower provider networks, limiting choice of doctors and hospitals.
- Potential for reduced quality of care if plans cut costs to compensate for overpayments.
Provider Perspectives on Inflated Benchmarks
Healthcare providers, including doctors, hospitals, and other healthcare facilities, also face consequences related to inflated benchmarks. While some providers might benefit from increased payments under the current system, the long-term sustainability of the system is questionable. Inflated benchmarks contribute to higher overall healthcare costs, potentially leading to reduced reimbursements in the future or stricter regulations. Moreover, the focus on maximizing payments based on inflated benchmarks can incentivize unnecessary services, ultimately harming patient care.
- Potential for reduced future reimbursements due to unsustainable spending.
- Increased administrative burden associated with navigating complex risk adjustment models.
- Incentives to provide unnecessary services to maximize payments.
Payer (Medicare Advantage Plan) Perspectives on Inflated Benchmarks
Medicare Advantage plans, the private insurers administering Medicare benefits, are caught in a complex situation. While inflated benchmarks initially lead to higher payments, the long-term consequences can be detrimental. Increased scrutiny and potential future reductions in payments could destabilize the financial viability of some plans. This could lead to consolidation within the industry or limit the availability of Medicare Advantage options for beneficiaries.
- Increased risk of financial penalties and future payment reductions.
- Pressure to maintain profitability amidst rising costs and increased scrutiny.
- Potential for decreased competitiveness and consolidation within the Medicare Advantage market.
Government Perspectives on Inflated Benchmarks
The government, ultimately responsible for the financial sustainability of Medicare, bears the brunt of inflated benchmarks. Overpayments represent a significant drain on taxpayer funds, impacting the overall budget and potentially diverting resources from other critical programs. The government’s perspective is driven by the need to ensure the long-term solvency of the Medicare program while maintaining access to quality care for beneficiaries.
- Significant increase in Medicare spending and budget deficits.
- Pressure to implement reforms to control costs and ensure program solvency.
- Need to balance cost containment with ensuring access to quality care for beneficiaries.
Future Research Directions: Medicare Advantage Overpayments Inflated Benchmarks Health Affairs
The analysis of Medicare Advantage overpayments, while revealing concerning trends, leaves significant gaps in our understanding. Further research is crucial to refine our models, improve payment accuracy, and ultimately ensure the financial integrity and equitable provision of healthcare for seniors. This requires a multi-faceted approach leveraging advanced data analytics and focusing on specific areas of uncertainty.The current methodologies used to calculate risk adjustment and benchmark payments need rigorous scrutiny.
While the Health Affairs article highlighted several limitations, a deeper dive into these methodological shortcomings is necessary to propose concrete improvements. Furthermore, the interplay between various factors contributing to overpayments—such as coding practices, beneficiary characteristics, and provider incentives—requires more comprehensive investigation.
Data Analytics for Payment Accuracy
Improving the accuracy of Medicare Advantage payment calculations hinges on leveraging advanced data analytics. Machine learning algorithms, for instance, could be employed to identify patterns and anomalies in claims data that suggest potential overpayments. This could involve developing predictive models that flag high-risk claims for further review, thereby improving the efficiency of audit processes. For example, an algorithm trained on historical data could identify unusual patterns in diagnosis codes or service utilization that correlate with inflated payments.
This proactive approach, rather than relying solely on reactive audits, would significantly enhance the accuracy and timeliness of payment adjustments.
Risk Adjustment Model Refinement
The current risk adjustment model, while aiming to account for differences in beneficiary health status, may not fully capture the complexity of individual needs. Future research should focus on refining this model to incorporate additional factors that influence healthcare costs. This might involve incorporating social determinants of health, such as socioeconomic status and access to care, into the risk adjustment calculations.
A more comprehensive model could potentially reduce the discrepancies between predicted and actual costs, thereby minimizing the potential for overpayments. For example, a study could compare the accuracy of a model incorporating social determinants of health data with the current model, measuring the reduction in prediction error.
Provider Incentive Alignment
Investigating the alignment of provider incentives with accurate coding and billing practices is essential. Future research could explore whether certain payment structures or incentive programs inadvertently encourage upcoding or other practices that lead to inflated payments. This research could involve comparing payment patterns across different provider types and payment models to identify potential correlations between incentive structures and overpayment rates.
For example, a study could compare the overpayment rates of providers participating in capitated versus fee-for-service models to assess the influence of payment mechanisms on coding practices.
Longitudinal Studies of Payment Trends
Longitudinal studies tracking payment trends over extended periods are crucial to understand the evolving dynamics of Medicare Advantage overpayments. These studies could provide valuable insights into the effectiveness of policy interventions and the long-term impact of changes in risk adjustment methodologies and provider incentives. By analyzing payment data over multiple years, researchers could identify emerging patterns and trends that might not be apparent in cross-sectional analyses.
For example, a longitudinal study could track the impact of a specific policy change on overpayment rates over a five-year period, allowing for a more comprehensive evaluation of its effectiveness.
Last Word
The issue of Medicare Advantage overpayments driven by inflated benchmarks is a complex one with far-reaching consequences. While the Health Affairs article provides crucial insights into the extent of the problem, much work remains to be done to fully understand the intricacies of risk adjustment, identify effective solutions, and ensure the long-term sustainability of Medicare. Ultimately, addressing this issue requires a multi-faceted approach involving policymakers, healthcare providers, and beneficiaries alike, working collaboratively to create a fairer and more efficient system that protects both taxpayers and beneficiaries.
Frequently Asked Questions
What are the potential consequences of these overpayments for Medicare beneficiaries?
While beneficiaries directly benefit from Medicare Advantage plans, inflated payments could lead to higher premiums or reduced benefits in the future if the program becomes unsustainable.
How are these inflated benchmarks affecting the private insurance companies involved?
The inflated benchmarks result in increased profits for many Medicare Advantage plans. However, this could lead to increased scrutiny and potential future regulatory changes.
What role does the government play in addressing this issue?
The Centers for Medicare & Medicaid Services (CMS) is responsible for overseeing Medicare Advantage and needs to implement stricter oversight and potentially revise payment methodologies.
Are there any ongoing efforts to reform the Medicare Advantage payment system?
Yes, there are ongoing debates and legislative efforts focused on reforming the risk adjustment model and improving payment accuracy in Medicare Advantage.




